
Original scientific article
Implementation of improved postoperative care decreases the mortality
rate of operated mice after an abundant 6-hydroxydopamine lesion of
nigrostriatal dopaminergic neurons
by Sini K. Koski, Sakari Leino, Saara Rannanpää and Outi Salminen
Division of Pharmacology and Pharmacotherapy, Faculty of Pharmacy,
University of Helsinki
 Correspondence: Outi Salminen,
Correspondence: Outi Salminen,
Division of Pharmacology and Pharmacotherapy,
Faculty of Pharmacy, University of Helsinki
Viikinkaari 5 (P.O. Box 56), 00014 University of Helsinki, Finland
Email: outi.salminen@helsinki.fi
Summary
A mouse model of Parkinson’s disease with an abundant lesion of
nigrostriatal dopaminergic neurons can be achieved by stereotactic
injection of 6-hydroxydopamine into the medial forebrain bundle.
However, postoperative mortality can be excessively high without
intensive postoperative care. Here, we show that improvements in
stereotactic operations and postoperative care result in significant
benefits for both animal well-being and research efficiency. Adopting
a wide combination of mostly previously described improvements
resulted in a decrease of postoperative mortality from 71% to 14% and
an increase in successful abundant dopaminergic lesions from 46% to
81%. The techniques adopted are described in detail. In addition, we
describe a simple protocol for gradual preoperative handling which can
be utilized to decrease animal stress, aggressive and aversive
behaviors, and to facilitate postoperative care and other subsequent
handling. We propose that the implementation of these improvements
greatly decreases the risk of animal suffering and that the
improvements are worth adopting in any research group utilizing
abundant 6-hydroxydopamine-induced dopaminergic lesions in mice.
Suggestions for further improvement are also presented.
Introduction
Various ways exist to establish rodent models of Parkinson’s disease, a neurodegenerative motor disorder caused by the death of dopaminergic neurons that have their cell bodies in the substantia nigra pars compacta (SNc) and project into the dorsal striatum. Neurodegeneration and motor symptoms of Parkinson’s disease can be mimicked in animals by degenerating these nigrostriatal neurons with different neurotoxins, administered either systemically or intracranially, or by genetic manipulations (Bové & Perier, 2012). Importantly, different methods can cause different degrees of neurodegeneration, which affects not only the severity of the parkinsonian symptoms but, in the case of intracranial neurotoxin injection models requiring stereotactic surgery, also the required intensity of postoperative care. Particularly in the case of abundant lesions, the time and commitment needed for postoperative care may surprise researchers new to the method.
This article focuses on a mouse model utilizing abundant unilateral
nigrostriatal lesions, where the neurotoxin 6-hydroxydopamine (6-OHDA)
is injected into the medial forebrain bundle (MFB) of one brain
hemisphere. When successful, this method of lesioning causes a loss of
over 90% of dopaminergic neurons in the ipsilateral SNc (Bové &
Perier, 2012). However the model leads to a transient severe
disturbance in motor coordination which can significantly hinder the
recovery of operated animals. In order to consistently achieve
successful and abundant dopaminergic neurodegeneration, along with low
postoperative mortality, we have during the past several years made
significant efforts to improve the MFB 6-OHDA lesion procedure as well
as the postoperative care.
The multiple adopted improvements can be divided into three main
categories which are 1) preoperative handling and care 2) operation
parameters and 3) postoperative care. Preoperative handling decreases
the experience of stress in mice and facilitates overall handling
related to e.g., postoperative care, drug injections and behavioral
tests. Improvements in operation parameters during surgery were
adopted, based on published methods(Thiele et al., 2011), to improve
the hit rate to the correct brain area as well as to minimize damage
to other brain areas. Most importantly, a broad combination of
improvements in postoperative care, adapted from descriptions in
various previous studies, greatly increased the proportion of
surviving animals.
Here, to provide a collated technical description of the various
available improvements, we describe in detail how to successfully
conduct a stereotactic 6-OHDA injection into the mouse MFB, how to
offer appropriate postoperative care, and how to facilitate handling
and increase well-being with preoperative handling. We also show that
adopting these improvements resulted in statistically significant
benefits for both animal well-being, decreasing average postoperative
mortality from 71% to 14%, and research efficiency, with the
proportion of successfully lesioned mice increasing from 46% to 81%.
Materials & Methods
Animals
Due to potential bias related to genetic manipulations, only studies
conducted with C57BL/6J mice from a commercial breeder (Harlan
Netherlands, Horst, Netherlands) or wild type mice of genetically
modified strains with a C57BL/6J background (maintained in The
Laboratory Animal Centre or Neuroscience Center and Institute of
Biomedicine, University of Helsinki, Helsinki, Finland) were included
in this study. Both sexes were used, but the use of female mice was
preferred to avoid penile prolapse complications. Separate studies had
different numbers of animals with different age and body weight
distributions. When possible, aged and thus more weighty mice were
used to lower the impact of postoperative weight loss. Mice obtained
from the commercial breeder were allowed at least several weeks of
acclimatization before the initiation of any experimental procedures.
Detailed information about the experimental animals is given in Table
1.
Table 1. Detailed information on the mice subjected to intra-MFB 6-OHDA injections.
|
Study group |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
N (total) |
28 |
17 |
6 |
15 |
10 |
20 |
12 |
14 |
Age (weeks) |
13–26 |
15–17 |
15 |
28 |
20–23 |
30 |
10–20 |
17–21 |
Weight (grams) |
20–33 |
22–29 |
18–26 |
23–31 |
20–25 |
21–36 |
21–24 |
20–28 |
Gender |
Both |
Females |
Both |
Females |
Females |
Females |
Females |
Females |
Strain |
C57BL/6J |
C57BL/6J |
C57BL/6J |
C57BL/6J |
C57BL/6J |
C57BL/6J |
C57BL/6J |
C57BL/6J |
Genotype |
α5 +/+ |
WT |
α5 +/+ |
WT |
α5 +/+ |
WT |
α5 +/+ |
HDC +/+ |
Source |
LAC |
HA |
LAC |
HA |
LAC |
HA |
LAC |
NC |
α5 = alfa5 nicotinic acetylcholine receptor subunit
HDC = histidine decarboxylase
HA = Harlan Netherlands, Horst, Netherland
LAC = Laboratory Animal Centre, University of Helsinki, Helsinki,
Finland
NC = Neuroscience Center and Institute of Biomedicine, University of
Helsinki, Helsinki, Finland
All mice were maintained in pathogen-free conditions according to FELASA 2014 recommendations (Mähler et al., 2014) and housed in individually ventilated plastic cages (GM500; cage dimensions,W x D x H, 391 x 199 x 160 mm; Tecniplast, Buguggiate, VA, Italy) with half of the cage covered by a wire bar food hopper. For enrichment, bedding (aspen chips, 5 x 5 x 1 mm, 4HP, Tapvei, Paekna, Harjumaa, Estonia), nesting material (aspen strips, PM90L, Tapvei, Paekna, Harjumaa, Estonia) and a brick (aspen brick, 100 x 20 x 20 mm, Tapvei, Paekna, Harjumaa, Estonia) were placed in the cages. Mice were kept in groups of three to six (with the exception of keeping males singly or in pairs when unavoidable due to fighting) under a 12/12h light-dark cycle with lights off at 18:00. The mice had free access to standard food pellets (Harlan Teklad 2916C; Harlan, Indianapolis, IN, USA) and filtered, UV-irradiated water. The ambient temperature was held at +23±2 °C and the relative humidity at 50±15%. Animal experiments were conducted according the 3R principles of the EU directive 2010/63/EU governing the care and use of animals used for scientific purposes, and subsequent local laws and regulations [Finnish Act on the Protection of Animals Used for Scientific or Educational Purposes (497/2013, Government Decree on the Protection of Animals Used for Scientific or Educational Purposes (564/2013)]. Study protocols were authorized by the national Animal Experiment Board of Finland (licence numbers ESAVI/198/04.10.07/2014, ESAVI/431/04.10.07/2015 and ESAVI/441/04.10.07/2016).
Preoperative handling and care
Introduction of preoperative handling was initiated with study group 2
and subsequently conducted with all animals. Handling of mice, aimed
at reducing the stress of animals and at facilitating postoperative
care and future handling, was initiated two to three weeks before
surgery and performed gradually within three to four days. The
researcher used the same protective overalls on each day to
familiarize the animals to the researcher’s odor.
On the first day of the preoperative handling the aim was to introduce
the researcher to the mice and to apply tail marks with a marker pen.
The mice were allowed to sniff the researcher’s gloves, first while
remaining under the nesting material and subsequently with the nesting
material removed. Concurrently, the researcher talked quietly to
familiarize the mice with the researcher’s voice. The mice were lifted
by their tail one at a time onto the researcher’s hand, which remained
in the cage to allow the mice to freely jump away.
On the second day, the actions described above were repeated, and
additionally the animals’ weights were measured and a new handling
protocol was introduced. Up to five mice were lifted onto the
researcher’s arm while standing close to the home cage; the mice had
the freedom to return to the home cage or sniff and explore the
researcher’s arm.
On the third day, the same protocol was performed as the day before,
but before lifting the animals from the tail to the researcher’s hand,
the researcher tried to move the mice by lifting from the body: the
researcher put his/her hand gently under the mouse, so that the mouse
was against the wall of the home cage, and the mouse was lifted gently
with the hand underneath the body.
On the last day, the same protocol was performed as described before,
but the mice were no longer lifted from the tail. Additionally,
petting (gently stroking the head and sides with a finger) was
initiated if the mice allowed it. In subsequent study phases, after
the mouse was habituated to non-tail lifting, it was always handled
and transferred by lifting from underneath the body, unless impossible
due to circumstances of the experiment being performed.
Additional preoperative actions were performed in preparation for the
operation itself and postoperative care. During preoperative handling
(2–3 weeks before surgery) a high calorie dietary supplement (Bacon
softies; Bio-Serv, Flemington, NJ, USA) was introduced, the standard
nesting material (aspen strips) replaced with soft cotton pads
(Nestlets, Article ref. 14010, Plexx, Elst, Netherlands), and a small
plastic house (Mouse House, Tecniplast, Buguggiate, VA, Italy) added
to every cage for additional enrichment. During each study there was
one responsible researcher assigned who took care of conducting the
experiments but also monitoring the animals, changing the animal cages
(once a week) and confirming that sufficient food was available. When
necessary, another researcher assisted the responsible researcher but
never replaced that person.
Stereotactic operation
The 6-OHDA MFB lesion procedure described below was developed on the
basis of previously published methods (Lundblad et al., 2004; Thiele
et al., 2011). A premedication of desipramine (25 mg/kg, i.p.) was
administered in certain studies (for more details, see Table 4) 30
minutes prior to injection of 6-OHDA to decrease 6-OHDA-induced damage
to noradrenaline and serotonin neurons. Buprenorphine (0.1 mg/kg, i.p)
was administered for pain relief 5 minutes prior isoflurane anesthesia
(4% induction, 0.5–2% maintenance, individually adjusted). The mouse
was then positioned into a stereotactic frame (Stoelting Co, Wood
Dale, IL, USA), the head was shaved, and an incision was made after
applying lidocaine local anesthesia. When the skull was exposed, a 10
µl syringe (NanoFil, World Precision Instruments Inc., Sarasota, FL,
USA) with a 33 G needle was filled with fresh 6-OHDA-solution (15
µg/µl, except in the first trial the concentration was 3 µg/µl) and
covered with aluminum foil. The needle was placed at the Bregma, the
Bregma was marked, and the needle moved to the Lambda. If the D/V
difference between the Bregma and Lambda was greater than ± 0.2, the
position of the animal’s head was adjusted and the Bregma and Lambda
checked again. The needle was then placed at the following coordinates
from Bregma: A/P -1.2 and M/L -1.1. A hole was made through the skull
using a drill (Foredom, Stoelting Co, Wood Dale, IL, USA) and the
needle inserted into the medial forebrain bundle at D/V -5.0. The
injection volume was 0.2 µl with a speed of 0.1 µl/min (except in the
first trial the volume was 1 µl with a speed of 0.5 µl/min), resulting
in administration of 3 µg 6-OHDA in total. After the injection, the
needle was left in place for 5 minutes and then slowly retracted
during 2 minutes. The wound was closed by two to three stitches and
0.5 ml of sterile and warm saline (NaCl 0.9%) was delivered
subcutaneously. Carprofen (5 mg/kg, s.c.) was administered for pain
relief after the operation, and the mouse was taken off the
stereotactic frame and placed in a warm recovery cage until regaining
consciousness. For further pain relief, buprenorphine was
re-administered 6 h after surgery and carprofen re-administered 20–24
h after surgery.
Postoperative care
Following surgery, the mice received 14 days of daily intensive
postoperative care (for a summary, see Table 2). If the mice showed
signs of hypothermia (shaking and still), the cage was placed on a
heating pad and kept there 4 to 6 hours, taking care to use a low
level of heating to provide a warmer cage while avoiding hyperthermia.
Small plastic houses and soft nesting material (cotton pads), already
added preoperatively, were also used to mitigate hypothermia. Mice
received 1 ml injections (s.c.) of sterile and warm saline twice daily
(maximum 10 days) to mitigate dehydration, and carprofen injections if
they showed signs of pain (e.g., vocalization, piloerection, ungroomed
appearance, aggression, lack of group behavior, abnormal posture or
shaking, immobilization, sunken eyes; National Research Council
Committee on Recognition and Alleviation of Pain in Laboratory
Animals, 2009). High calorie dietary supplements, Bacon softies
(Bio-Serv, Flemington, NJ, USA), Nutrigel (Virbac, Carros, France) and
Nutri-plus Gel (ClearH2O®, Portland, ME, USA) were provided to
compensate for difficulties in eating and weight decrease. Body weight
and behavior (signs of dehydration, activity, eating, drinking) were
systematically monitored using a specific welfare scoring table
(Appendix 1).
If needed, the mice were fed by hand twice daily with water provided
directly into the mouth via a 1 ml syringe (for video material, see
Appendices 2 and 3). In some cases a more active and forceful feeding
was necessary. This was achieved by holding the mouse in an
intraperitoneal injection position (grasping from the neck scruff and
lifting the belly towards the researcher) and approaching the mouth
with a tiny spoon filled with Nutri-plus Gel. The mouth was touched
with the spoon and eating was monitored. When feeding in this way,
particular attention should be paid to ensure that the angle of the
spoon is optimal with respect to the tongue and jaw movements of the
mouse.
Genitals of male mice were checked every day in order to detect any
signs of developing penile prolapse (redness and swelling of the
penis). If penile prolapse was observed, it was immediately treated by
rinsing the genital area with sterile warm water, applying honey-based
wound care ointment (Vetramil, FaunaPharma, Espoo, Finland) and gentle
massage of the bladder area. Despite intensive postoperative care,
some individual mice did not recover and needed to be sacrificed based
on humane endpoint criteria described in Table 3 and Appendix 1.
Data analysis
Mice that underwent the 6-OHDA lesion surgery were divided into the
following categories: Alive (mice that were successfully lesioned and
survived the postoperative period), Dead (mice that died during
postoperative care), Dead in Surgery (mice that died during the
operation), Unlesioned (mice that were unsuccessfully lesioned).
Lesion success was determined post mortem on the basis of tyrosine
hydroxylase (dopaminergic neuron marker) immunostaining of the
substantia nigra pars compacta, performed after a variable time from
surgery (ranging from 1.5 to 6 months) depending on the specific study
in question.
The postoperative mortality rate (%) was calculated as the ratio of
mice that died during postoperative care vs. all successfully lesioned
animals (Dead / Alive + Dead). Mice that died during surgery and
unsuccessfully lesioned mice were not included. The rate of successful
lesioning (%) was calculated as the ratio of successfully lesioned
mice vs. all mice that survived (Alive / Alive + Unlesioned).
The statistical significance of the differences in the postoperative
mortality rate and the rate of successful lesioning before vs. after
the introduction of improvements was investigated with Pearson’s
Chi-Square tests.
Table 2. Improvements in utilization of the medial forebrain bundle
6-hydroxydopamine mouse model.
Actions during different experimental phases before and after the
introduction of the improvements.
|
Phase |
Before improvements |
After improvements |
|
Whole study |
||
Participants |
Several researchers conduct the experiments |
Designated researcher responsible for carrying out the whole
experiment |
|
Preoperative |
||
|
Mice
Nesting material
Housing
Handling |
Young mice preferred
Woody nesting material
Housed randomly
No handling by the researcher before operation |
Aged and weighty (bodyweight not less than 20 g) mice
preferred
Woody nesting material replaced with soft nesting material
Gradually proceeding handling protocol to habituate the mice to the researcher |
|
During surgery |
||
|
Isoflurane anesthesia
6-OHDA infusion volume
6-OHDA infusion speed |
Isoflurane kept at 1.5 – 2% as regularly advised
2 µl
0.5 µl/min |
Isoflurane kept as low as possible (0.5 – 2%) without reappearance of reflexes
Decreased infusion volume: 0.2 µl
Slower infusion speed: 0.1 µl/min |
|
Postoperative care |
||
|
- Duration
- Welfare checks
- Nutrition
- Body temperature
- Rehydration
- Penile prolapse |
Care provided for 1–2 weeks during weekdays only
Welfare not assessed or recorded systematically
Softened laboratory standard food placed on the bottom of the cage
No action
Warm and sterile saline and/or glucose delivered s.c. once a day when necessary
No proactive actions to avoid penile prolapse |
Care provided for 14 successive days, also during weekends
Welfare scored daily with a specific table
Softened standard food covered with Nutri-plus gel and placed in
a cup on the bottom of the cage
Hypothermic mice kept in a warmed cage 4–6 h daily
Warm and sterile saline (1 ml) delivered s.c. 1–2 times a day for max. 10 days
Genitals of male mice checked daily and signs of penile prolapse treated immediately |
Table 3. Determination of humane endpoints for MFB-lesioned mice. The mice were monitored daily for 14 successive days after the operation and offered intensive postoperative care. In addition to an immediate endpoint of over 25% loss of weight, systematic scoring of well-being was performed using a welfare scoring table to assess eating, drinking and activity, with mice euthanized if a set score was exceeded (see Appendix 1).
|
Weight monitoring (immediate endpoint) |
Over 25% loss of weight |
|
Eating and drinking (included in welfare scoring) |
|
Mouse is not eating when hand-fed |
|
Mouse is not drinking when watered via syringe |
|
Mouse is dehydrated: skin is not retracted following skin pinch and eyes are sunk in the head |
|
Activity (included in welfare scoring) |
|
Mouse is not moving spontaneously, frozen and/or shaking |
Results
Effects of preoperative handling and care
The effects of the gradual handling protocol described above were not
systematically investigated, but the introduction of the preoperative
handling led to what appeared to the researchers to be obvious and
significant reductions in - or even complete abolishment of -
aggressive and escape behaviors such as biting, jumping, vocalization
and general aversion towards the researcher, as well as to greatly
facilitated subsequent handling due to voluntarily approaching the
researcher and accepting physical restraint. See Appendix 4 for video
material (mice previously handled with the above protocol) supporting
the above observations. Furthermore, urination and defecation when
handled, a measure of stress and anxiety in mice (Hurst & West,
2010), were markedly decreased or even abolished.
Preoperative handling proved particularly useful in facilitating the
postoperative care procedures requiring fine coordination such as
injection administration and hand feeding and watering (see Appendices
2 and 3 for video of hand feeding and watering). In addition,
preoperative handling facilitated all later stages of the individual
studies, allowing easy performance of procedures such as drug
administration and behavioral experiments as well as quick and
stress-free euthanasia by cervical dislocation.
Postoperative mortality and lesion success
A timeline for the introduction of the different improvements is shown
in Figure 1. Table 4 lists the postoperative mortality and the
proportion of successful abundant dopaminergic lesions within the
different study groups as well as the average before and after
improvement introduction. Average postoperative mortality was greatly
reduced after the introduction of the systematic welfare scoring along
with the other improvements (between studies 1 and 2), decreasing from
71% to 14%. The difference in postoperative mortality was
statistically highly significant (χ2(1) =
27.8, P = 1.3E-7, Pearson Chi-Square test). Euthanized mice
accounted for most of the mortality. Before the implementation of the
improvements, a few spontaneously dying (i.e., not euthanized) mice
were observed during the period of postoperative care; after the
implementation, spontaneously dying mice were very rare (one animal in
total). Concurrently, improvements in surgical procedures increased
the average rate of successful abundant lesions from 46% to 81%. The
difference in successful lesions was statistically significant
(χ2(1) = 7.45, P = 0.006).
|
|
Figure 1. Timeline of the different improvements introduced. Individual studies are listed in chronological order on the
left side of the arrow and improvements are listed on the right
side of the arrow. Click image to enlarge |
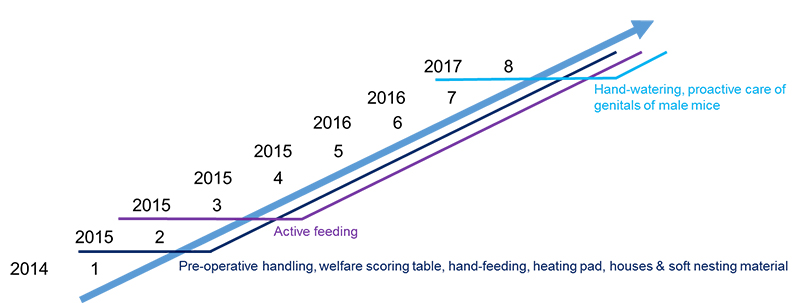
Table 4. Significant decrease in postoperative mortality after the introduction of welfare scoring and other improvements. Alive = only successfully lesioned mice included, Dead = died during postoperative care, †Surgery = died during operation, Unlesioned = based on tyrosine hydroxylase immunostaining of the substantia nigra pars compacta. Postoperative mortality% = Dead / Alive + Dead, Successfully lesioned% = Alive / Alive + Unlesioned
|
Study group |
Alive |
Dead |
†Surgery |
Unlesioned |
n (total) |
Postoperative mortality (%) |
Successfully lesioned (%) |
Exceptions in surgery protocol |
1A |
2 |
11 |
0 |
3 |
16 |
85 |
40 |
Desipramine, |
1B |
4 |
4 |
0 |
4 |
12 |
50 |
50 |
Desipramine |
|
Total - Before improvements |
6 |
15 |
0 |
7 |
28 |
71 |
46 |
|
2 |
9 |
2 |
2 |
4 |
17 |
18 |
69 |
|
3 |
3 |
1 |
0 |
2 |
6 |
25 |
60 |
Desipramine |
4 |
12 |
1 |
0 |
2 |
15 |
8 |
86 |
|
5 |
5 |
2 |
1 |
2 |
10 |
29 |
71 |
|
6 |
17 |
1 |
0 |
2 |
20 |
6 |
89 |
|
7 |
9 |
2 |
1 |
0 |
12 |
18 |
100 |
Desipramine |
8 |
9 |
1 |
1 |
3 |
14 |
10 |
75 |
|
|
Total - After improvements |
64 |
10 |
5 |
15 |
94 |
14 |
81 |
|
Discussion
Modeling late-stage Parkinson’s disease in mice can be challenging, as an abundant toxin-induced nigrostriatal lesion often leads to transient but severe motor disturbances, even in the case of the typically utilized unilateral lesions that affect only one brain hemisphere. Reaching acceptable levels of postoperative survival can thus require quite intensive care. Here, we have described the technical details and impact of improvements in postoperative care and other techniques related to the MFB 6-OHDA mouse model that have been adopted in our research group during the past several years. The improvements consisted of a combination of mostly previously described techniques (see Table 5), and as shown have markedly increased the proportion of surviving animals. The postoperative care and other methodology described here thus comprises a stable and reliable combination of methods to achieve significant improvements in the proportion of surviving animals as well as the well-being of the animals. However, it must be stressed that refinement of animal experiments is a continuing process, and many possibilities for further improvement remain.
The achievement of these results is likely to be due to the sum of all
improvements made rather than any specific improvement. While direct
comparison of survival rates with previously reported MFB model mouse
studies is difficult, as a number of studies have not described in
detail the methods used for postoperative care or humane endpoints
(e.g., the maximum loss of weight allowed) or the specifics of how
reported survival and/or mortality rates were calculated, the achieved
average survival rate of 86% closely resembles the survival rate
reported recently by a number of other groups utilizing multifaceted
postoperative care (Table 5). However, as 100% survival rates after an
abundant dopaminergic lesion have been reported by at least one
research group (Francardo et al., 2011; Sebastianutto et al., 2016),
further improvement remains possible. Note also that while
postoperative survival is obviously critical for research purposes and
easy to quantify, other measures of animal well-being could allow for
the evaluation of further and possibly more subtle refinement. Each of
the different improvements described here, as well as some
opportunities for further improvement, will next be discussed.
Table 5. Descriptions of postoperative care and survival rate after MFB 6-OHDA lesions in mice from selected methodological articles. ND = not described
|
Reference |
Hand-feeding |
Supplemental nutrition |
Rehydration |
Monitoring well-being, criteria for sacrifice |
Treatment of penile prolapse |
Ensuring sufficient body temperature |
Duration of postoperative care |
Group housing |
Survival rate (6-OHDA dose) |
|
Lundblad |
ND |
ND |
ND |
ND |
ND |
ND |
ND |
ND |
18% (3 µg) |
|
Cenci & Lundblad 2007 |
Yes |
Food soaked in sugar/water solution |
Glucose-saline solution (s.c.) |
Weak mice separated from healthy mice. Mice that remain weak and drowsy sacrificed. |
ND |
ND |
2–3 weeks, |
ND |
ND |
|
Francardo |
Yes |
Food soaked in sugar/water solution |
Glucose-saline solution (s.c.) 1st week daily, continuation as necessary |
Weaker mice separated from healthy mice. |
ND |
ND |
1–3 weeks, |
ND |
80–100% (3.2 µg) |
|
Thiele et al., 2011 |
ND |
Nutrigel, kitten milk replacement, sugared water |
Lactated Ringer’s solution (s.c.) |
Weight, movement, food and water intake and presence and consistency of fecal matter monitored. |
Lubricating jelly to the penis, palpitation of the bladder and rehydration. |
ND |
2 weeks daily |
Yes |
82% (3 µg) |
|
Glajch et al., 2012 |
ND |
Pediasure |
Saline (s.c.) daily |
Grooming and overall appearance monitored. |
ND |
Continuously on a heating pad (35 °C) |
ND |
ND |
85% (2.5 µg) |
|
Heuer et al., 2012 |
ND |
Wet food |
Glucose-saline solution (s.c.) |
Weight monitored, if below 85 % need for euthanasia evaluated |
ND |
ND |
2 weeks |
Yes |
83% (6 µg) |
|
Heuer et al., 2013 |
ND |
Wet food |
Glucose-saline solution (s.c.) |
Body weight monitored |
ND |
ND |
2 weeks |
Unclear |
93% (6 µg) |
|
Boix et al., 2015 |
Yes |
Food soaked in sugar/water solution, DietGel Boost |
Glucose-saline solution (s.c.) |
ND |
ND |
ND |
2 weeks |
ND |
80% (3.6 µg) |
|
Sebastianutto et al., 2016 |
ND |
DietGel Boost |
Glucose/ |
ND |
ND |
Overnight in warm ventilated cabinet (30 °C) for 1 week |
2–3 weeks |
ND |
100% (3.2 µg) |
Selection of animals for the study should naturally be primarily based
on scientific justifications. However, in our experience as old and
weighty mice as possible should be chosen when justified, because the
higher starting weight confers partial protection from the transient
but marked weight decrease typically associated with an abundant
nigrostriatal lesion. In addition, it may be preferable to select
female mice, as they are not affected by the penile prolapse
complications which can affect male mice after a severe dopaminergic
lesion (Thiele et al., 2011) and can also be more easily group housed
due to less fighting. It should naturally be kept in mind that the
study design may prevent the inclusion of only female mice due to
possible gender-specific confounds such as the estrus cycle.
Animals were group housed whenever possible, not only due to stress
caused by social isolation, but also to mitigate hypothermia. Nesting
material was changed from woody material to soft material, and plastic
houses provided, in an effort to mitigate hypothermia. The soft
nesting material is also easier for the mice to manipulate even in a
weakened state. It should also be mentioned that the regular aspen
strip nesting material in use at our facilities has a tendency to be
become coated with the gel-like dietary supplement materials used in
postoperative care and get stuck to the mice, sometimes even causing
constrictive injury. All changes to the housing conditions were
performed 2–3 weeks before surgery to allow habituation. Further
improvement could be achieved by introducing the housing changes even
earlier, ensuring full habituation.
Related to the entire study process, we have aimed at assigning one
primary researcher to be responsible for the entire experiment, with
assistance from other researchers when necessary. In particular,
during the experiment (beginning from preoperative handling) the
primary researcher is responsible for all handling of the animals
e.g., during cage changes. While we have not systematically studied
the effects of handling by one vs. several persons, we suggest that
this is likely to increase the animals’ habituation to the
researcher’s smell, voice and handling practices and thus to reduce
the stress the mice experience.
The introduction of the gradual handling protocol appeared to be very
effective in reducing aggressive and anxiety-related behaviors in the
mice and facilitating subsequent handling as well as postoperative
care. Nevertheless, the handling protocol could surely be further
improved. One possibility for further improvement could be to begin
non-aversive (non-tail) handling immediately on day one, instead of
beginning with tail handling. Another improvement would be to avoid
the disruption of nests during handling.
A limitation of the present study is that the effects of preoperative
handling were not systematically studied. However, for a demonstration
of the effects of the handling protocol see the included video
material (Appendix 4), where a distinct lack of aversive behaviors
directed towards the researcher as well as markedly easy handling can
be observed. See also Appendices 2 and 3 demonstrating that the
pre-handled mice accept hand-feeding and watering after surgery. Also
note that very similar pre-experimental handling has been previously
described by Fridgeirsdottir et al. (2014), who observed improved
performance and less variability in handled mice in the Morris water
maze task, likely due to reduced stress and anxiety. Different
handling methods have also been previously studied in mice and found
to affect the voluntary interaction with the researcher even with
brief exposure. The common method of picking up and restraining the
mouse by its tail was found to induce aversion, high anxiety and no
habituation even after many handling sessions, while non-aversive
handling methods such as lifting the mouse with cupped hands (similar
to our method of handling) or using a tunnel resulted in low anxiety,
voluntary approach and acceptance of restraint (Ghosal et al., 2015;
Gouveia & Hurst 2017; Hurst & West 2010). Our observations of
greatly reduced anxiety-like and aversive behaviors are thus in full
concordance with previous literature. In addition, utilizing a
combination of “massage” (resembling our petting technique) and
non-aversive handling was found to reduce stress-related plasma
corticosterone increases in response to a novel environment (Ghosal et
al., 2015). This finding suggests that the reductions in aversive
behaviors observed – in the literature as well as in the present study
– are mirrored by a reduced physiological stress response.
Our improvements to the surgical protocol included lower isoflurane
maintenance anesthesia (0.5 – 2%) as well as decreased 6-OHDA infusion
volume and speed. The use of a lower isoflurane concentration was
adopted to promote faster recovery from anesthesia. It is critically
important, however, that deep enough anesthesia is maintained to
ensure no experience of pain. The depth of anesthesia (e.g., absence
of reflexes) must therefore be carefully monitored at all times. The
reduced 6-OHDA infusion volume and speed were adopted to minimize
damage to structures close to the MFB, such as the hypothalamus which
regulates feeding and drinking behavior (Thiele et al., 2011). These
improvements were also likely to contribute to the significantly
increased proportion of successful lesions, which in turn allows for a
reduction in the total number of animals needed.
Perhaps the most critical steps taken with respect to the increased
postoperative survival rate were improvements in postoperative care.
Intensive postoperative care is crucial and should be applied daily
for at least two weeks. Care should naturally be continued for longer
if needed – however, we suggest that a cut-off time be considered if
mice continue to require intensive care for longer than two weeks.
Note also that even more frequent (e.g., twice daily) observation and
care may be necessary, particularly if spontaneously dying animals are
encountered.
Unilateral lesioning of the MFB leads to severe but transient motor
coordination problems due to the massive dopaminergic cell death
affecting one hemisphere. Thus, obvious problems in motor control of
tongue, chin and forepaws can often be observed, and in practice it
appears that the animals need to relearn how to use one side of their
body after an abundant lesion. It should be stressed, however, that
despite the near-total nigrostriatal lesion of one brain hemisphere,
surviving animals regain their gross motor coordination abilities
after two or more weeks of intensive care and are able to move, eat
and drink as normal, with remaining parkinsonian symptoms typically
revealed only by specific behavioral tests or under pharmacological
stimulation.
Postoperative supplementary nutrition is essential to ensure adequate
food intake, and survival, in the most severely affected mice. We have
used several types of commercial high-energy palatable food pellets
and gels, with a number of other commercial products used successfully
by others (see Table 5). The supplementary foods were introduced
before surgery to habituate the animals. During postoperative care,
supplementary food gels were also hand-fed to animals showing severe
difficulties in eating and drinking or, often, to all animals.
Drinking water was also hand-fed, and warm saline injected daily to
further mitigate dehydration. Note that others have also successfully
used saline/glucose or Ringer solution injections for hydration (see
Table 5). Further essential improvements in postoperative care
included careful monitoring for symptoms of hypothermia and keeping
hypothermic mice in a warmed cage, and careful monitoring of genitalia
of male mice to enable treatment of any developing penile prolapse
before it reached a severe stage. Further improvement could be
achieved by keeping all operated mice at constant thermoneutrality (30
°C for mice; Fischer et al., 2018) using more advanced
thermostat-regulated heating devices, instead of utilizing
non-regulated heating pads and only for limited amounts of time per
day.
It is necessary to emphasize that every mouse used is an individual
and it is highly important to observe them individually. A successful
abundant nigrostriatal lesion leads most notably to transient weight
loss. However, while weight loss is an indicator of well-being, and
often utilized as an objective humane endpoint criterion, the entirety
of the behavior and appearance of the animal should be taken into
account when assessing well-being. At times, it can be very clear that
the mouse exhibiting the most severe weight loss (as % of initial
weight) is not the mouse suffering the most. For instance, while in
our studies an animal that reaches a weight loss of more than 25% of
initial weight is sacrificed, as stipulated by our animal use permit,
in the same cage there might be an animal that remains immobile and is
obviously suffering despite having lost only 15–20% of its weight. To
facilitate the monitoring of animal well-being we have therefore
developed a systematic method using a specific welfare scoring table
(Appendix 1). This is used to record animal weight and behavior and to
determine whether a humane endpoint has been reached for each
individual animal. It should also be noted that opportunities for
further improvements in humane endpoints and the monitoring and
assessment of individual animal condition (including the welfare
scoring system) undoubtedly exist. Additional improvements could
include systematic consideration of gradual vs. precipitous weight
loss, measurements of food and water intake, monitoring of breathing,
or following body temperatures with methods such as subcutaneously
implanted RFID (radio-frequency identification) chips or infrared
thermometry (Mei et al., 2018). Note, however, that changes in motor
activity after surgery should in general not be considered as humane
endpoints (excluding dramatic changes such as being frozen or
shaking), given that motor dysfunction is an essential feature of the
parkinsonian animal model and can be particularly but temporarily
pronounced during the postoperative period, including in animals that
will fully recover. On the other hand, re-establishment of normal
motor activity such as nest building could be considered a sign of
recovery.
In conclusion, in this article we have provided a collated technical
description of a number of mostly previously described improvements
related to the utilization of the MFB 6-OHDA mouse model of
Parkinson’s disease. We show that the implementation of these
improvements resulted in significant increases in both postoperative
survival and successful abundant nigrostriatal dopaminergic lesions.
We suggest that this combination of improvements also greatly
decreases the risk of animal suffering and is worth adopting in any
research group utilizing or planning to utilize the MFB 6-OHDA model.
Finally, we stress that refinement of animal experiments is a
continuing process, and there remain many opportunities for further
improvement – both those few suggested above as well as probably many
others.
Acknowledgement and funding
The authors would like to thank Anna Peltonen, Raisa Hänninen, Ceren Pajanoja and Sara Figuerola Santamonica for their participation in the surgery and postoperative care described in this article. All studies were funded by a grant from the Academy of Finland (1267761) to Outi Salminen, with additional funding provided by the Finnish Parkinson Foundation.
References
- Boix, J., Padel, T., Paul G., (2015). A partial lesion model of Parkinson’s disease in mice - Characterization of a 6-OHDA-induced medial forebrain bundle lesion. Behavioural Brain Research. 284, 196-206.
- Bové, J., Perier, C., (2012). Neurotoxin-based models of Parkinson’s disease. Neuroscience. 211, 51–76.
- Cenci, M.A., Lundblad, M., (2007). Ratings of L-DOPA-induced dyskinesia in the unilateral 6-OHDA lesion model of Parkinson’s disease in rats and mice. Current Protocols in Neuroscience. 41, 9.25.1-9.25.23.
- Fischer, A.W., Cannon, B., Nedergaard, J., (2018). Optimal housing temperatures for mice to mimic the thermal environment of humans: An experimental study. Molecular Metabolism. 7, 161-170.
- Francardo, V., Recchia, A., Popovic, N., Andersson, D., Nissbrandt, H., Cenci, M.A., (2011). Impact of the lesion procedure on the profiles of motor impairment and molecular responsiveness to L-DOPA in the 6-hydroxydopamine mouse model of Parkinson’s disease. Neurobiology of Disease. 42, 327-340.
- Fridgeirsdottir, G.A., Hillered, L., Clausen, F., (2014). Escalated handling of young C57BL/6 mice results in altered Morris water maze performance. Upsala Journal of Medical Sciences. 119, 1-9.
- Glajch, K.E., Fleming, S.M., Surmeier, D.J., Osten, P., (2012). Sensorimotor assessment of the unilateral 6-hydroxydopamine mouse model of Parkinson’s disease. Behavioural Brain Research. 230, 309-316.
- Ghosal, S., Nunley, A., Mahbod, P., Lewis, A.G., Smith, E.P., Tong, J., D’Alessio, D.A., Herman, J.P., (2015). Mouse handling limits the impact of stress on metabolic endpoints. Physiology & Behavior. 150, 31-37.
- Gouveia, K., Hurst, J.L., (2017). Optimising reliability of mouse performance in behavioural testing: The major role of non-aversive handling. Scientific Reports. 7, 44999.
- Heuer, A., Smith, G.A., Lelos, M.J., Lane, E.L., Dunnett, S.B., (2012). Unilateral nigrostriatal 6-hydroxydopamine lesions in mice I: Motor impairments identify extent of dopamine depletion at three different lesion sites. Behavioural Brain Research. 228, 30-43.
- Heuer, A., Smith, G.A., Dunnett, S.B., (2013). Comparison of 6-hydroxydopamine lesions of the substantia nigra and the medial forebrain bundle on a lateralised choice reaction time task in mice. European Journal of Neuroscience. 37, 294-302.
- Hurst, J.L., West, R.S., (2010). Taming anxiety in laboratory mice. Nature Methods. 7, 825-826.
- Lundblad, M., Picconi, B., Lindgren, H., Cenci, M.A., (2004). A model of L-DOPA-induced dyskinesia in 6-hydroxydopamine lesioned mice: Relation to motor and cellular parameters of nigrostriatal function. Neurobiology of Disease. 16, 110-123.
- Mei, J., Riedel, N., Grittner, U., Endres, M., Banneke, S., Emmrich, J.V., (2018). Body temperature measurement in mice during acute illness: implantable temperature transponder versus surface infrared thermometry. Scientific Reports. 8, 3526.
- Mähler, M., Berard, M., Feinstein, R., Gallagher, A., Illgen-Wicke, B., Pritchett-Corning, K., Raspa, M., (2014). FELASA recommendations for the health monitoring of mouse, rat, hamster, guinea pig and rabbit colonies in breeding and experimental units. Laboratory Animals. 48, 178-192.
-
National Research Council (US) Committee on Recognition and
Alleviation of Pain in Laboratory Animals, (2009). Recognition and
alleviation of pain in laboratory animals., Washington, D.C., USA:
National Academies Press.
Sebastianutto, I., Maslava, N., Hopkins, C.R., Cenci, M.A., (2016). Validation of an improved scale for rating L-DOPA-induced dyskinesia in the mouse and effects of specific dopamine receptor antagonists. Neurobiology of Disease. 96, 156–170. - Thiele, S.L., Warre, R., Khademullah, C.S., Fahana, N., Lo, C., Lam, D., et al. (2011). Generation of a model of L-DOPA-induced dyskinesia in two different mouse strains. Journal of Neuroscience Methods. 197, 193–208.
Appendices
Appendix 1.
PDF: Welfare scoring table
Appendix 2.
Video material: Delivery of supplemental food by hand
Appendix 3.
Video material: Delivery of drinking water by hand
Appendix 4.
Video material: Behavior of mice handled previously with the gradual
handling protocol