
Original scientific article
Buprenorphine, but not lidocaine, effectively attenuates post-operative thermal hypersensitivity in an incisional model in neonatal rats (Rattus norvegicus)
by Erin M Katz1, Monika K Huss1*, Katechan Jampachaisri2, Cholawat Pacharinsak1
1Department of Comparative Medicine, Stanford University, Stanford,
CA
2Department of Mathematics, Naresuan University, Phitsanulok,
Thailand
 Correspondence: Monika Huss, email: monikag@stanford.edu
Correspondence: Monika Huss, email: monikag@stanford.edu
Summary
There is limited information on safe and effective neonatal rodent analgesia. The aim of this study was to evaluate the efficacy and duration of analgesia provided by buprenorphine (Bup) and lidocaine (Lid) in an incisional pain model. Male and female postnatal day three Sprague Dawley rat pups (n=40) were randomly assigned to one of five treatment groups: 1) Saline - 0.1 ml subcutaneous (SC)/0.01 ml saline incisional infiltration; 2) BupL - 0.025 mg/kg Bup, SC/0.01 ml saline infiltration; 3) BupH - 0.05 mg/kg Bup, SC/0.01 ml saline infiltration; 4) LidL - 2 mg/kg lidocaine infiltration/0.1 ml saline SC; and 5) LidH - LDC 4 mg/kg lidocaine infiltration/0.1 ml saline SC. Rat pups were anesthetized with sevoflurane by mask, and a 1-cm full thickness skin incision was made over the left lateral thigh. Infiltration of lidocaine or saline occurred prior to wound closure with surgical glue. Baseline thermal latency was measured 24 hr prior to surgery, and subsequently 1, 2, 4, 8, 24, and 48-hrs post-operatively using an infrared diode laser. Thermal latency in the Saline group was significantly reduced compared to baseline up to the 4 hr timepoint. Both BupL and BupH attenuated thermal hypersensitivity for at least 4 hours in this model. LidL attenuated thermal hypersensitivity for 1 hr and LidH failed to attenuate thermal hypersensitivity. No abnormal clinical signs were noted for all treatment groups throughout the study. In summary, a single pre-operative dose of buprenorphine 0.025 to 0.05 mg/kg (SC) effectively attenuated postoperative thermal hypersensitivity in 3-day old neonatal rat incisional pain model for 4 hours.
Introduction
Prior to 1985, it was widely thought that neonatal rodents were unable to experience pain because of an underdeveloped nervous system and analgesia was not routinely provided during neonatal surgical procedures (McLaughlin and Dewey 1994). It is now widely recognized that neonatal rodents are reactive to a painful stimulus and that uncontrolled pain experienced by neonates leads to long-term behavioral changes (Van Sluyters and Obernier 2004; Barr et al. 1992; Blass et al. 1993; Fanselow and Cramer 1988; Liu et al. 1997; Anand et al. 1999). Providing analgesia to neonates is difficult because of their physiological differences from adults which affect drug absorption, distribution, metabolism and elimination (Van Sluyters and Obernier 2004; Ku and Smith 2015) . Although it was previously shown that opioids such as fentanyl may provide effective analgesia in neonates, they have a short duration of action (under 30 min for fentanyl), necessitating frequent administration and stress related handling (Flecknell 2016). Buprenorphine, when used in adult rats provides a duration of action of 8-12 hrs, and if buprenorphine can also be safely and effectively used in neonatal rats it would reduce the need for frequent administration of other analgesics such as fentanyl for neonates (Pacharinsak and Smith 2017). Because of these challenges, limited information on analgesic techniques for neonatal rodents is available despite the fact they are used for stereotaxic (Cetin et al. 2006; Chambers et al. 1996; Cunningham and McKay 1993; Davidson et al. 2010), spinal (Hu et al. 1997), cardiovascular (Porrello et al. 2011; Porrello et al. 2013), thoracic (Frimpong-Boateng and Surh 2013), laparoscopic (Hary et al. 1986), reproductive (Hary et al. 1986) and dermal (Boon et al. 1992) surgical procedures. Rodent neonatal analgesia has been an area of increased consideration in laboratory animal medicine. Providing neonates with perioperative analgesics is crucial for animal welfare and consistent experimental outcomes (Turner et al. 2016).
Opioids are a mainstay analgesic with buprenorphine being most commonly used for rodent models (Christoph et al. 2005; Guarnieri et al. 2012). Opioids, such as buprenorphine and morphine, have abundant receptors throughout the body which can lead to numerous side effects including sedation, respiratory depression, bradycardia, emesis, constipation, and urinary retention (Benyamin et al. 2008). Although physiological side effects are not the focus of this current study, there is increased concern with the use of opioids in neonates because of their known respiratory sensitivity and immature central nervous system (Schlossmann 1937; Kupferberg and Way 1963; Way et al. 1965; Marsh et al. 1997). Previous research in neonatal dogs confirmed sensitivity to the sedative and respiratory effects of opioids (Luks et al. 1998). Another study in 3-day rat pups indicated that while morphine, meperidine, fentanyl and buprenorphine were effective antinociceptive agents, cardiovascular sensitivity was seen with buprenorphine (McLaughlin and Dewey 1994). Although buprenorphine is commonly used in adult rats, little is known about recommended dosage, safety and effectiveness when used in neonatal rodents for surgical procedures.
Other commonly used rodent analgesics are local anesthetics and non-steroidal anti-inflammatory drugs (NSAIDs). Although NSAIDs can provide good analgesia, they are not recommended in neonates with immature hepatorenal systems (Kohn 1997). Local anesthetics, such as lidocaine, are useful for managing acute pain providing a 1-hour duration of action (Khan et al. 2002). Lidocaine hydrochloride is used in human neonates for acute pain (Lehr and Taddio 2007). Unlike opioids, lidocaine is not a controlled substance and has the advantage of providing local anesthesia while causing fewer systemic side effects (Lehr and Taddio 2007). Lidocaine has also been used in veterinary medicine for some neonatal species including pigs, dogs and cats (Lomax et al. 2017), however published use in neonatal rodents is limited. As lidocaine is considered safe and easy to use, (Golzari et al. 2014; Essink-Tjebbes et al. 1999) we sought to also evaluate its potential as an analgesic for surgical procedures in neonatal rats. Because of the longer duration of action provided by buprenorphine and the ease of use of lidocaine, the current study investigated the effectiveness of these two analgesics at attenuating post-operative hypersensitivity in neonatal rat pups.
In this study, we examined the analgesic effect of buprenorphine and lidocaine on post-operative thermal hypersensitivity in a minor pain procedure lasting 4 hours. The aim was to investigate whether a single dose of buprenorphine (low or high dose) or a single dose of lidocaine (low or high dose) would effectively attenuate post-operative thermal hypersensitivity in an incisional pain procedure in 3-day old rat pups.
Materials & Methods
Animals and housing conditions
Postnatal day three (P3) Sprague Dawley rats [(Crl: CD (SD) IGS),
(n=40, 20 male, 20 female), Charles River Laboratories,
Hollister, CA] were used. Pups arrived at the facility on P1. They
were housed in litters of 10 pups per dam in static microisolator
cages (Allentown, Inc., Allentown, NJ) on ALPHA-dri paper bedding
(Shepherd Specialty Papers, Milford, NJ). Rooms were maintained on a
12:12 h light:dark cycle, between 70 to 74°F (21 to 23°C), and 30 to
70% relative humidity. Rat dams were fed a commercial diet (Teklad
Global 18% Protein Rodent Diet 2018, Harlan Laboratories, Madison, WI)
and were provided bottles of reverse osmosis filtered water
ad libitum. Rats were free of rat coronavirus, rat Theiler
virus, Kilham rat virus, rat parvovirus, Toolan H1 virus, rat minute
virus, lymphocytic choriomeningitis virus, murine adenovirus types 1
and 2, reovirus type 3, Sendai virus, pneumonia virus of mice,
Mycoplasma pulmonis, mites, lice and pinworms.
Neonatal rats were assessed daily for weight gain, nursing, and
inclusion in the maternal nest. All experiments were approved by the
Stanford Administration Panel for Laboratory Animal Care. All
rats were treated in accordance with the
Guide for the Care and Use of Laboratory Animals in a
facility accredited by the Association for the Assessment and
Accreditation of Laboratory Animal Care, International.
Study design
The researchers were blinded to the experimental groups. Two pups per litter (4 litters) were randomly assigned to one of five treatment groups (n=10 equal male and female pups per group): 1) Saline, 0.1 ml, subcutaneous route (SC) (0.9% NaCl, Hospira, Lake Forest, IL) + 0.01 ml incisional infiltration; 2) low dose buprenorphine – BupL, 0.025 mg/kg, SC (buprenorphine HCl, 0.3 mg/ml, Par Pharmaceutical, Chestnut Ridge, NY) + 0.01 ml saline incisional infiltration; 3) high dose buprenorphine – BupH, 0.05 mg/kg, SC + 0.01 ml saline incisional infiltration; 4) low dose lidocaine – LidL, 2 mg/kg, incisional infiltration (2% lidocaine HCl, VetOne, MWI Animal Health, Boise, ID) + 0.1 ml saline, SC; 5) high dose lidocaine – LidH, 4 mg/kg, incisional infiltration + 0.1 ml saline, SC. All doses of buprenorphine and saline were administered subcutaneously in the intrascapular region using 1 ml 25 g 5/8” tuberculin syringes (Monoject, Covidien, Dublin, Ireland). Incisional infiltration of lidocaine and saline were topically splashed on the edges of the incisions prior to closure.
Anesthesia and surgical model
All surgical procedures were performed between 0900 and 1000. General anesthesia was induced in P3 rats using sevoflurane (Sevothesia, Henry Schein, Dublin, OH) with 100% oxygen in an induction chamber (2L/min of 100% O2 with 8% sevoflurane). Anesthesia was maintained with a modified nose cone by applying a glove and cutting a circular hole for the nose (500 mL/min of 100% O2 with sevoflurane 4-8%). Anesthetic depth was monitored via respiratory rate, mucous membrane color, and hindlimb paw withdrawal. Thermal support was provided via circulating warm-water blanket set to 38°C (Stryker T/Pump, Portage, Michigan). Upon induction, subcutaneous experimental agents were administered in the intrascapular region consistent with the respective treatment group. The neonate was placed in right lateral recumbency and the left thigh was aseptically prepared with three alternating scrubs of betadine (10% povidone-iodine, Purdue Products L.P., Stamford, CT) and 70% Isopropyl Alcohol USP (Henry Schein, Melville, NY). A 1-cm full thickness skin incision was made over the left lateral thigh (No. 15 blade, Swann-Morton, Sheffield, England). Local infiltration into the incision site with the experimental treatment group was then performed. The incision was approximated and closed with surgical adhesive (VetOne, MWI, Boise, ID). The surgery lasted up to five minutes. Sevoflurane was stopped and pups were supplied with 100% oxygen for 1-minute before being further recovered in an un-bedded recovery cage over a warm water circulating blanket. Once fully recovered, pups were returned to the dam.
Thermal hypersensitivity
Baseline measurements were performed 24 h prior to surgery (P2) and then 1, 2, 4, 8, 24, and 48-h postoperatively (post-surgery). Thermal hypersensitivity was evaluated using an infrared diode laser stimulator (LASS-10 M, LASMED, Mountain View, CA). The laser diode was set at 480 mA and held 7 cm from the skin to focus the beam to a 5-mm diameter circular focus point aimed directly on the thigh skin incision. Before testing, skin temperature of the thigh was assessed using an infrared thermometer (Kintrex Infrared Thermometer IRT0421, Kintrex, Vienna, VA) prior to all measurements. Thermal hypersensitivity was measured as thermal latency, i.e. the time (seconds) to withdraw the hind limb during laser stimulation. A maximum thermal exposure of 19 seconds was used to prevent tissue injury. Two measurements were recorded at a minimum of 2 min apart, for the ipsilateral and contralateral thighs. During testing, thermal support was provided by a warm water circulating blanket. Thermal hypersensitivity was defined as a significant (P < 0.05) decrease in thermal latency.
Statistical analysis
Body weight, ipsilateral and contralateral skin temperature and thermal latency were analyzed using ANOVA with repeated measures followed by Bonferroni for multiple comparisons (SPSS, IBM, Somers, NY). Data are expressed as mean ± SEM. Data were tested for normality. A p-value of less than 0.05 was considered as significant.
Results
Body weight
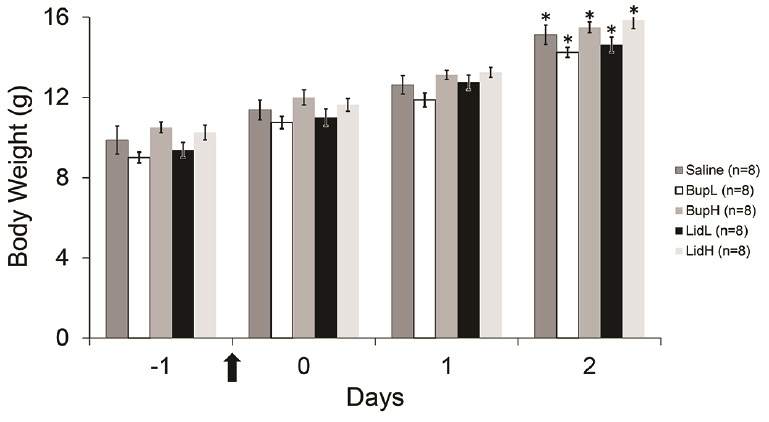
There were no differences between sexes; therefore, data were combined (Figure 1). Baseline (day -1) body weights of rat pups in the Saline (9.9 ± 0.4 g), BupL (9 ± 0.3 g), BupH (10.5 ± 0.3 g), LidL (9.4 ± 0.4 g), and LidH (10.3 ± 0.4 g) groups were not significantly different from each other (Figure 1). The body weights of rat pups on the last day of the experiment (day 2) in Saline (15.1 ± 0.5 g; p<0.001), BupL (14.3 ± 0.3 g; p<0.001), BupH (15.5 ± 0.3 g; p<0.001), LidL (14.6 ± 0.4 g; p<0.001) and LidH (15.9 ± 0.4 g; p<0.001) groups were significantly higher than those on the first day of the experiment (day -1).
|
|
Figure 1. Baseline body weights (day -1) of
neonatal rats, on day of surgery (day 0), day after surgery (day
1) and 2 days following surgery (day 2). Arrow indicates time of
surgery. *, Value is significantly (P < 0.05)
different from -24 hr (baseline) for all treatment groups after
analyses using repeated measure with Bonferroni for multiple
comparisons. Click image to enlarge |
Thermal latency
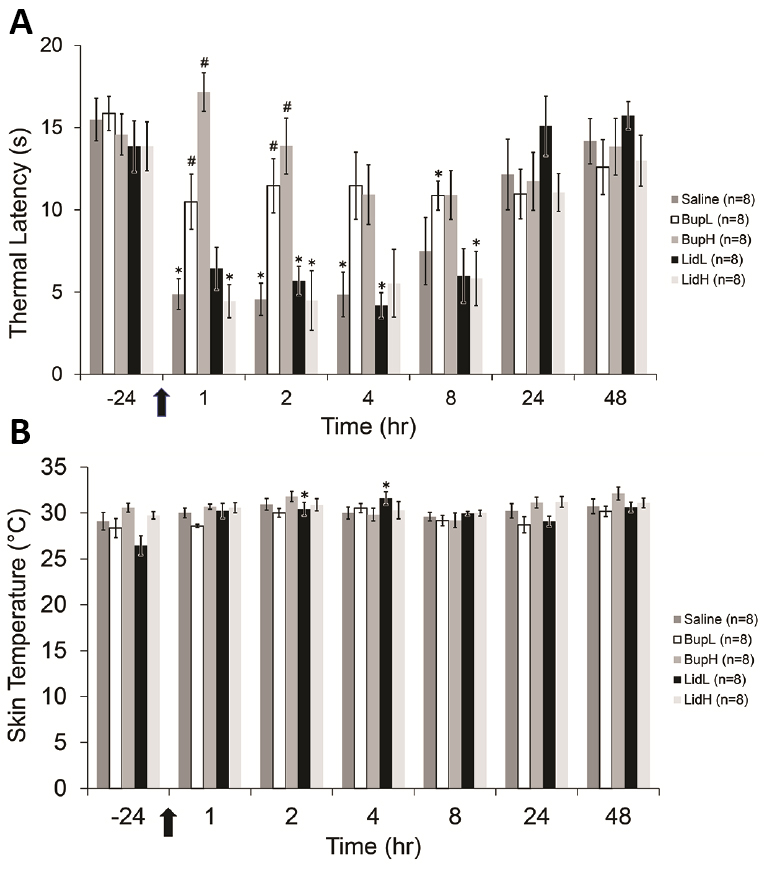
There were no differences seen between sexes; therefore, data was again combined. Thermal latency did not differ at -24 hr (before surgery) between groups [Saline (15.5 ± 1.3 s), BupL (15.9 ± 1.0 s), BupH (14.6 ± 1.3 s), LidL (13.8 ± 1.6 s), and LidH (13.9 ± 1.5 s) (Figure 2A). In the ipsilateral thigh, thermal latency of rat pups in the Saline group significantly decreased at 1 [4.9 ± 0.9 s; p<0.001], 2 [4.6 ± 1.0 s; p<0.001], and 4 [4.8 ± 1.4 s; p<0.001] hr after surgery compared with baseline values (-24 hours before surgery). Compared to -24 hr values, thermal latency of rat pups in the BupL group only significantly decreased at 8 [10.9 ± 0.9 s; p<0.001] hr while thermal latency of rat pups in the BupH group did not differ at any time points. Compared to baseline values, thermal latency of rat pups in the LidL group significantly decreased at 2 [5.7 ± 0.9 s; p=0.003] and 4 [4.2 ± 0.8 s; p<0.001] hr while thermal latency of rat pups in the LidH group significantly decreased at 1 [4.4 ± 1.0 s; p<0.001], 2 [4.5 ± 1.8 s; p=0.003], and 8 [5.8 ± 1.7 s; p=0.003] hr. Compared to the Saline group, the thermal latency of rat pups in the BupL and BupH group significantly increased at 1 hr [10.49± 1.68 s, p=0.030, and 17.15± 1.17 s, p<0.001), respectively] and 2 hrs [11.46± 1.65 s, p=0.020, and 13.88± 1.70 s, p<0.001, respectively] but not at later time points. Thermal latency on the contralateral thigh (see Figure 2B) did not differ at any time points in any of the groups from their baseline measurement [there was no overall effect of treatment on the contralateral thigh; (p=0.159)].
|
|
Figure 2A (Ipsilateral Thigh). Thermal hypersensitivity (measured as thermal latency [s] to withdrawal; mean ± SEM) of the ipsilateral thigh [treatment, F(4, 35)=4.20, p=0.007; time, F(4.7, 164.1)=32.75, p<0.001; interaction between the 2 factors, F(18.8, 164.1)=4.69, p<0.001]. Arrow indicates time of surgery. *Values significantly (P < 0.05) different from the -24 hr (baseline) value for the same treatment group. #Values significantly (P < 0.05) different from the saline group after analyses using ANOVA with repeated measures followed by Bonferroni for multiple comparisons. Figure 2B (Contralateral Thigh). Thermal sensitivity (measured as thermal latency [s] to withdrawal; mean ± SEM) of the contralateral thigh [treatment, F(4, 35)=1.76, p=0.159; time, F(4.2, 146.4)=3.19, p=0.014; interaction between the 2 factors, F(16.7, 146.4)=1.89, p=0.024].. Arrow indicates time of surgery. *Values significantly (P < 0.05) different from the -24 hr (baseline) value for the same treatment group after analyses using repeated measure with Bonferroni for multiple comparisons.
Click image to enlarge |
Skin temperature
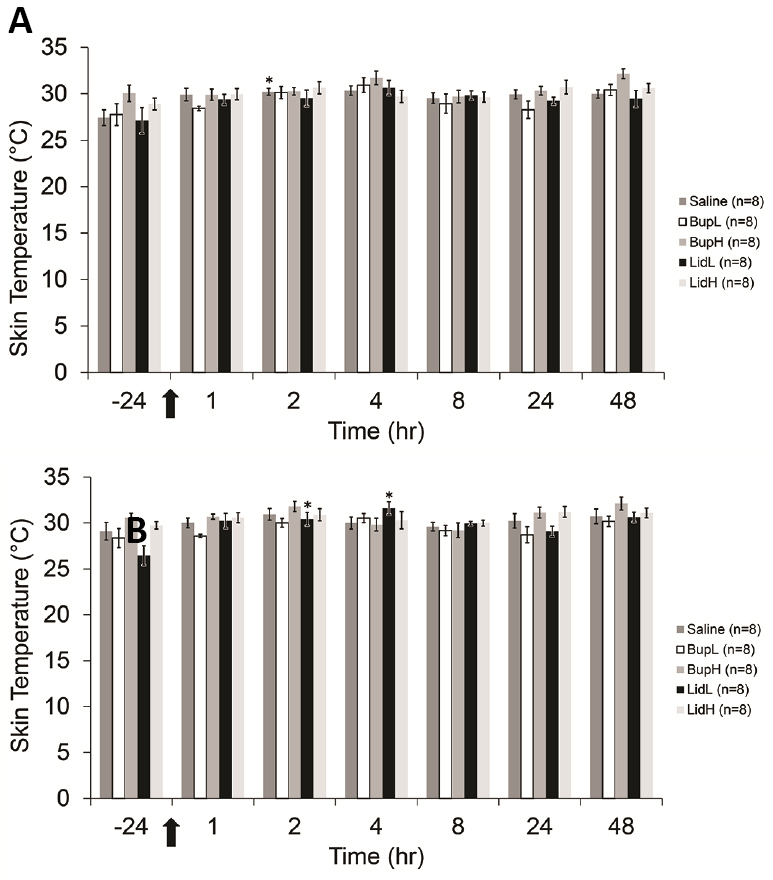
There were no differences seen between sexes; therefore, data was again combined. In the ipsilateral thigh, skin temperature did not differ at baseline (-24 hrs before surgery) between all groups [Saline (27.4 ± 0.8 °C), BupL (27.8 ± 1.2 °C), BupH (30 ± 0.9 °C), LidL (27.1 ± 1.4 °C), and LidH (28.9 ± 0.6 °C)] (Figure 3A). In Saline group, skin temperature was significantly higher at 2 [30.2 ± 0.4 °C; p=0.003] hr compared to baseline values (-24 hours before surgery). In other groups, skin temperature did not differ at any time points. In the contralateral thigh, skin temperature did not differ at -24 hr (before surgery) for all groups [Saline (29.1 ± 1.0 °C), BupL (28.4 ± 1.0 °C), BupH (30.6 ± 0.5 °C), LidL (26.5 ± 1.1 °C), and LidH (29.7 ± 0.4 °C)] (Figure 3B). In LidL group, skin temperature was significantly higher at 2 [30.4 ± 0.7 °C; p=0.002] and 4 [31.6 ± 0.7 °C; p<0.001] hr compared to baseline values (-24 hrs before surgery). In other groups, skin temperature did not differ at any time point.
|
|
Figure 3A (Ipsilateral Thigh). Skin temperature of the ipsilateral thigh measured in degrees Celsius (°C; mean ± SEM) [treatment, F(4, 35)=4.89, p=0.005; time, F(4.2, 145.3)=6.48, p<0.001; interaction between the 2 factors, F(16.6, 145.3)=0.83, p=0.651]. Arrow indicates time of surgery. *Values significant (P < 0.05) different from the -24 hr (baseline) value for the same treatment group after analyses using repeated measure with Bonferroni for multiple comparisons. Figure 3B (Contralateral Thigh). Skin temperature of the contralateral thigh measured in degrees Celsius (°C; mean ± SEM) [treatment, F(4, 35)=6.05, p<0.001; time, F(6, 210)=6.06, p<0.001; interaction between the 2 factors, F(24, 210)=1.46, p=0.085]. Arrow indicates time of surgery. *Values significant (P < 0.05) different from the -24 hr (baseline) value for the same treatment group after analyses using repeated measure with Bonferroni for multiple comparisons.
Click image to enlarge |
Discussion
This study demonstrates that a single dose of buprenorphine, BupL (0.025 mg/kg, SC) or BupH (0.05 mg/kg, SC), effectively attenuates post-operative thermal hypersensitivity with an onset within 1 hr of administration and a duration of at least 4 hr. While LidL effectively attenuated post-operative thermal hypersensitivity for 1 hr, LidH did not attenuate thermal hypersensitivity during the first 2 hr post-surgery. Weights of rat pups in all treatment groups increased gradually and the weights on the last day of the experiment (day 2) were significantly higher than those on the baseline day (-24 hrs). To our knowledge, this is the first study demonstrating that buprenorphine effectively attenuates thermal hypersensitivity using a laser diode in rat pups.
Our lab has extensive experience with an incisional pain model using the plantar surface of a hind paw to imitate minor pain in rats (McKeon et al. 2011; Seymour et al. 2016; Kang et al. 2017; Chum et al. 2014; Zude et al. 2020). For this study we were using neonatal rats with much smaller hind paws than adults, thus a modified model involving skin incision of the thigh was chosen to increase the surgical area and assist with post-operative hypersensitivity testing. This approach was previously used by our lab to evaluate anesthetic depth in neonatal rat pups and adult rats (Huss et al. 2016; Heng et al. 2020). The contralateral thigh was also tested to serve as an un-injured control during testing. Previous work indicated that a diode laser provides sufficient stimuli to elicit a withdrawal reflex to test thermal hypersensitivity in adult rats (Tzabazis et al. 2005). In this study, we used a laser diode positioned 7 cm from the skin in order to get a beam focused on the surgical site of 5 mm. We determined our setting and maximum cut off time based on previous experience with adult rats and mice and other neonatal studies (Johnson et al. 1992; Cuellar et al. 2010). Using this technique, we found thermal hypersensitivity within 1 hr of surgery that lasted for 4 hrs in the Saline group indicating that the thigh incisional pain model produced a thermal hypersensitivity for at least 4 hrs in rat pups.
Skin temperature can affect thermal hypersensitivity measurement (Pertovaara et al. 1996), therefore, prior to testing at each time point we measured the skin temperatures of ipsilateral and contralateral thighs. We found that the skin temperatures within all groups was approximately 30°C throughout testing. Almost all skin temperatures were consistent with baseline temperature (-24 hr) aside from measurements in the Saline group at 2 hr on the ipsilateral thigh and LidL group at 2 and 4 hr on the contralateral thigh. The increase in skin temperature seen in the LidL group is unlikely to be attributed to the effect of lidocaine because it was seen on contralateral thighs. One potential explanation for the higher skin temperature could be situational from the uneven environmental warming. Although rat pups were placed sternally in a testing cage, they sometimes would move into a lateral recumbency which may cause the skin temperature to be higher on the recumbent legs. Additionally, throughout testing, pups were chosen randomly from their home cage and some pups were nested in the bedding or underneath the dam which could lead to uneven skin temperature distribution on the thigh. We were not able to acclimate rat pups to the cage because we were concerned about the rapid heat loss from being out of the nest and away from the dam. Therefore, once rat pups were placed in the testing cage, their skin temperatures were measured immediately. These could be potential explanations for variations in skin temperature during testing.
We expected that lidocaine would attenuate thermal hypersensitivity for the first 1-2 hrs as the reported duration of action ranges from 1 to 3 hr in veterinary species (Foley 2017; Garcia 2015; Perkowski and Wetmore 2006). A previous study in adult male rats undergoing a tail nerve block with 0.4 cc of 1% lidocaine, indicated that thermal and mechanical nociception was attenuated for 150±18 min and 115±10 min, respectively (Li et al. 2013). Our results indicated that for the thigh incisional pain model in neonatal rats, LidL attenuated thermal hypersensitivity for 1 hr and LidH failed to attenuate thermal hypersensitivity. Previous research using 0.5% bupivacaine doses scaled to body weight for sciatic nerve blockade, found that the duration of effectiveness was almost half as short in infant rats compared to adult rats (Hu et al. 1997). The recommended lidocaine dose for rodents is variable and the dose chosen for this study was based on doses (1-4 mg/kg) used in adult rats (Mert and Gunes 2012, Mert et al. 2013). To our knowledge, no studies have evaluated the effect of age on the duration of action of lidocaine. Possible explanations for the lack of attenuation seen include that the doses used were too low for the rat pups or because the duration of action was less than 1 hr. Although epinephrine is known to potentiate analgesic effects of lidocaine (Swain et al. 2017), we chose not to use lidocaine with epinephrine because of the neonates’ sensitivity to adverse effects. In future studies, additional earlier timepoints should be evaluated to determine lidocaine’s duration of action in neonates. The method of administration should also be considered as in this current study, a splash block technique was used to administer lidocaine before wound closure. Although the authors performed the splash block carefully, some drug solution might have leaked out of a surgical area leading to a lack of thermal hypersensitivity attenuation. While more challenging for neonates, future studies could also consider performing an incisional line block.
Opioids are commonly used to provide analgesia to human neonates (Hall and Shbarou 2009). Because buprenorphine is considered the gold standard in laboratory animals especially rodents, the authors decided to also evaluate the effectiveness of buprenorphine. In neonates, opioid doses are typically decreased by half of an adult dose in order to reduce negative side effects (Luks et al. 1998). Buprenorphine was previously reported to provide a dose-dependent antinociceptive effect during formalin and tail-flick test in 3-day old rat pups (Kitchen and Crowder 1985). With this in mind, the authors chose to evaluate two doses of buprenorphine, low (BupL, 0.025 mg/kg) and high (BupH, 0.05 mg/kg). Our results indicated that both BupL and BupH effectively attenuated thermal hypersensitivity for at least 4 hr in this model. We did not find alterations of thermal sensitivity thresholds in the contralateral side when buprenorphine was administered. A chronic or longer pain model is necessary to determine appropriate dosage intervals in rat pups. The authors believe that if a longer duration of pain model is used, buprenorphine may show longer attenuation of hypersensitivity. Because of the known side effects that buprenorphine causes in adult rats, clinical signs including respiratory depression and sedation, pruritus, weight loss, and maternal acceptance were monitored throughout the study. No adverse clinical signs were noted throughout the study following administration of either BupL or BupH.
In general, pre-operative analgesia (so called preventive analgesia) is always encouraged whenever possible during surgical procedures (Dahl and Kehlet 2011). Providing pre- and/or peri-operative analgesia not only prevents persistent post-operative pain, but also reduces the anesthetic requirements and leads to a smoother recovery. Providing preventive analgesia in neonates is also encouraged for the same reasons. Although we were not able to evaluate ultrasonic vocalizations we did evaluate the overall welfare and general appearance of the pups post-procedure which are more consistent indicators of overall pain in rodents (Williams et al. 2008; Turner et al. 2019). Pain level assessments of the pups post-surgery included assessing maternal acceptance (key for the pups survival), nursing, weight gain and the appearance of pain behaviors such as guarding, ambulation, and weight shifting (Turner et al. 2019). All pups were accepted by the dam, had consistent weight gain and no evidence of pain behaviors.
A limitation of this study was that we evaluated only thermal and not mechanical hypersensitivity as we found it very difficult to consistently measure a mechanical response in the neonates. Although both mechanical and thermal nociception are present in P1 rats, the sensitivity to the pain stimulus differs with age. Evaluation of thermal hypersensitivity using hot plate in P5 rats found that rat pups exhibited increased thermal but not mechanical hypersensitivity compared to adults (Hu et al. 1997). Mechanical hypersensitivity testing (von Frey monofilament) was not performed because during a pilot study von Frey monofilament testing was impractical and inconsistent. A hot water tail withdrawal assay showed that the thermal nociceptive threshold in neonatal rats is significantly lower than that of the adult rat until P12 and increased thermal hypersensitivity is observed up to P15 (Falcon et al. 1996). We also were not able to evaluate the pharmacokinetics of the plasma concentration of buprenorphine or lidocaine in the pups. Another limitation is that in this study, we did not combine both buprenorphine and lidocaine or administer lidocaine before making the incision to evaluate multimodal and pre-emptive analgesia which could also provide a longer duration and more complete analgesic regime for neonates. We did not evaluate fentanyl as a control group as we were seeking to evaluate a long-acting analgesic option for rodent neonates. Buprenorphine is a moderate opioid analgesic which may not fully attenuate thermal nociception in more invasive surgical models that involve more extensive tissue manipulation or visceral pain when compared to full m opioid agonists such as morphine (Gades et al. 2000; Bethesda 2012). A study of multimodal analgesics in neonatal rat pups is still needed. An additional limitation of the study was that long-term welfare assessments were not performed post-surgery to evaluate the long-term effects of providing a lack of analgesia.
In summary, we found that a single dose of either BupL (0.025 mg/kg, SC) or BupH (0.05 mg/kg, SC) was effective at attenuating post-operative thermal hypersensitivity in 3-day old rat pups for 4 hours. LidL (2 mg/kg) effectively attenuated thermal hypersensitivity for 1 hr in 3-day old rat pups. When choosing an analgesic for surgical procedures in neonatal rodents, factors to consider include the duration and severity of pain that is expected. Future studies should continue to evaluate the effectiveness of analgesics, including multimodal analgesics, in neonatal rodents using a model which causes sustained thermal hypersensitivity.
Acknowledgements
We are grateful to the assistance of Ms Janis Atuk-Jones in formatting and reviewing the manuscript. This study was supported by the Department of Comparative Medicine at Stanford University.
Conflict of interest
The authors declared no potential conflict of interest.
References
-
Anand, K.J., Coskun, V., Thrivikraman, K.V., Nemeroff, C.B., Plotsky, P.M., (1999). Long-term behavioral effects of repetitive pain in neonatal rat pups. Physiology & Behavior. 66, 627-637.
-
Barr, G.A., Miya, D.Y., Paredes, W., (1992). Analgesic effects of intraventricular and intrathecal injection of morphine and ketocyclazocine in the infant rat. Brain Research. 584, 83-91.
-
Benyamin, R., Trescot, A.M., Datta, S., Buenaventura, R., Adlaka, R., Sehgal, N., Glaser, S.E., Vallejo, R., (2008). Opioid complications and side effects. Pain Physician. 11, S105-1120.
-
Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases, (2012). LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. https://www.ncbi.nlm.nih.gov/books/NBK547852/
-
Blass, E.M., Cramer, C.P., Fanselow, M.S., (1993). The development of morphine-induced antinociception in neonatal rats: a comparison of forepaw, hindpaw, and tail retraction from a thermal stimulus. Pharmacology Biochemistry Behavior. 44, 643-649.
-
Boon, L., Manicourt, D., Marbaix, E., Vandenabeele, M., Vanwijck, R., (1992). A comparative analysis of healing of surgical cleft lip corrected in utero and neonates. Plastic and Reconstructive Surgery. 89, 11-17, discussion 18-20.
-
Cetin, A., Komai, S., Eliava, M., Seeburg, P.H., Osten, P., (2006). Stereotaxic gene delivery in the rodent brain. Nature Protocols. 1, 3166-3173.
-
Chambers, R.A., Moore, J., Mcevoy, J.P., Levin, E.D., (1996). Cognitive effects of neonatal hippocampal lesions in a rat model of schizophrenia. Neuropsychopharmacology. 15, 587-594.
-
Christoph, T., Kögel, B., Schiene, K., Méen, M., De Vry, J., Friderichs, E., (2005). Broad analgesic profile of buprenorphine in rodent models of acute and chronic pain. European Journal of Pharmacology. 507, 87-98.
-
Chum, H.H., Jampachairsri, K., Mckeon, G.P., Yeomans, D.C., Pacharinsak, C., Felt, S.A., (2014). Antinociceptive effects of sustained-release buprenorphine in a model of incisional pain in rats (Rattus norvegicus). Journal of the American Association for Laboratory Animal Science. 53, 193-197.
-
Cuellar, J.M., Manering, N.A., Klukinov, M., Nemenov, M.I., Yeomans, D.C., (2010). Thermal nociceptive properties of trigeminal afferent neurons in rats. Molecular Pain. 6, 39.
-
Cunningham, M.G., McKay, R.D., (1993). A hypothermic miniaturized stereotaxic instrument for surgery in newborn rats. Journal of Neuroscience Methods. 47, 105-114.
-
Dahl, J.B., Kehlet, H., (2011). Preventive analgesia. Current Opinion Anaesthesiology. 24, 331-338.
-
Davidson, S., Truong, H., Nakagawa, Y., Giesler, G.J.Jr., (2010). A microinjection technique for targeting regions of embryonic and neonatal mouse brain in vivo. Brain Research. 1307, 43-52.
-
Essink-Tjebbes, C.M., Hekster, Y.A., Liem, K.D., Van Dongen, R.T., (1999). Topical use of local anesthetics in neonates. Pharmacy World Science. 21, 173-176.
-
Falcon, M., Guendellman, D., Stolberg, A., Frenk, H., Urca, G., (1996). Development of thermal nociception in rats. Pain. 67, 203-208.
-
Fanselow, M.S., Cramer, C.P., (1988). The ontogeny of opiate tolerance and withdrawal in infant rats. Pharmacology Biochemistry Behavor. 31, 431-438.
-
Flecknell, P.A., (2016). Laboratory animal anaesthesia. Amsterdam; Boston, Elsevier/AP, Academic Press is an imprint of Elsevier.
-
Foley, P., (2017). Pain Management. In: Handbook of Laboratory Animal Anesthesia and Pain Management: Rodents. Eds: Pacharinsak, C., Smith, J.C. Boca Raton: CRC Press.
-
Frimpong-Boateng, K., Surh, C., (2013). Neonatal thymectomy prolongs the permeability of enteric antigens and promotes the strong activation of peripheral CD4 T cells (P3258). The Journal of Immunology. 190(Suppl.), 136.11.
-
Gades, N.M., Danneman, P.J., Wixson, S.K., Tolley, E.A., (2000). The Magnitude and Duration of the Analgesic Effect of Morphine, Butorphanol, and Buprenorphine in Rats and Mice. Contemporary Topics in Laboratory Animal Science. 39, 8-13.
-
Garcia, E.R., (2015). Local anesthetics. In: Veterinary Anesthesia and Analgesia: The Fifth Edition of Lumb and Jones. Eds: Grimm, K. A., Lamont, L. A., Tranquilli, W.J., Greene, S.A., Robertson, S.A. Wiley Blackwell.
-
Golzari, S.E., Soleimanpour, H., Mahmoodpoor, A., Safari, S., Ala, A., (2014). Lidocaine and pain management in the emergency department: a review article. Anesthesiology and pain medicine. 4, e15444-e15444. doi:10.5812/aapm.15444
-
Guarnieri, M., Brayton, C., Detolla, L., Forbes-McBean, N., Sarabia-Estrada, R., Zadnik, P., (2012). Safety and efficacy of buprenorphine for analgesia in laboratory mice and rats. Lab Animal (NY). 41, 337-43.
-
Hall, R.W., Shbarou, R.M., (2009). Drugs of choice for sedation and analgesia in the neonatal ICU. Clinics in perinatology. 36, 15-26.
-
Hary, L., Dupouy, J.P., Gregoire, I., (1986). Effects of castration and testosterone on the pituitary and adrenal responses of the newborn rat to ether inhalation. Neuroendocrinology. 42, 137-142.
-
Heng, K., Marx, J.O., Jampachairsi, K., Huss, M.K., Pacharinsak, C., (2020). Continuous Rate Infusion of Alfaxalone during Ketamine-Xylazine Anesthesia in Rats. Journal of the American Association for Laboratory Animal Science. 59, 170-175.
-
Hu, D., Hu, R., Berde, C.B., (1997). Neurologic evaluation of infant and adult rats before and after sciatic nerve blockade. Anesthesiology. 86, 957-965.
-
Huss, M.K., Chum, H.H., Chang, A.G., Jampachairsi, K., Pacharinsak, C., (2016). The Physiologic Effects of Isoflurane, Sevoflurane, and Hypothermia Used for Anesthesia in Neonatal Rats (Rattus norvegicus). Journal of the American Association for Laboratory Animal Science. 55, 83-88.
-
Johnson, C.A., Densen, P., Hurford, R.K. Jr, Colten, H.R., Wetsel, R.A., (1992). Type I human complement C2 deficiency. A 28-base pair gene deletion causes skipping of exon 6 during RNA splicing. Journal of Biological Chemistry. 267, 9347-9353.
-
Kang, S.C., Jampachaisri, K., Seymour, T.L., Felt, S.A., Pacharinsak, C., (2017). Use of Liposomal Bupivacaine for Postoperative Analgesia in an Incisional Pain Model in Rats (Rattus norvegicus). Journal of the American Association for Laboratory Animal Science. 56, 63-68.
-
Khan, M.A., Gerner, P., Sudoh, Y., Wang, G.K., (2002). Use of a charged lidocaine derivative, tonicaine, for prolonged infiltration anesthesia. RegIonal Anesthesia & Pain Medicine. 27, 173-179.
Kitchen, I., Crowder, M., (1985). Assessment of the hot-plate antinociceptive test in mice. A new method for the statistical treatment of graded data. Journal of Pharmacological Methods. 13, 1-7.
-
Kohn, D.F., (1997). Anesthesia and analgesia in laboratory animals. San Diego, Academic Press.
Ku, L.C., Smith, P.B., (2015). Dosing in neonates: special considerations in physiology and trial design. Pediatric Research, 77, 2-9.
Kupferberg, H.J., Way, E.L., (1963). Pharmacologic basis for the increased sensitivity of the newborn rat to morphine. Journal of Pharmacology and Experimental Therapeutics. 141, 105-112.
-
Lehr, V.T., Taddio, A., (2007). Topical anesthesia in neonates: Clinical practices and practical considerations. Seminars in Perinatology, 31, 323-329.
-
Li, Z., Chai, Y., Gong, C., Du, G., LIiu, J., Yang, J. (2013). Evaluation of the antinociceptive effects of lidocaine and bupivacaine on the tail nerves of healthy rats. Basic and Clinical Pharmacology and Toxicology. 113, 31-36.
-
Liu, D., Diorio, J., Tannenbaum, B., Caldji, C., Francis, D., Freedman, A., Sharma, S., Pearson, D., Plotsky, P.M., Meaney, M.J., (1997). Maternal care, hippocampal glucocorticoid receptors, and hypothalamic-pituitary-adrenal responses to stress. Science. 277, 1659-1662.
-
Lomax, S., Harris, C., Windsor, P.A., White, P.J. (2017). Topical anaesthesia reduces sensitivity of castration wounds in neonatal piglets. PLOS ONE. 12, e0187988. https://doi.org/10.1371/journal.pone.0187988
-
Luks, A.M., Zwass, M.S., Brown, R.C., Lau, M., Chari, G., Fisher, D.M., (1998). Opioid-induced analgesia in neonatal dogs: pharmacodynamic differences between morphine and fentanyl. Journal of Pharmacoogy and Experimental Therapeutics. 284, 136-141.
-
Marsh, D.F., Hatch, D J., Fitzgerald, M., (1997). Opioid systems and the newborn. British Journal of Anaesthesia. 79, 787-795.
-
McKeon, G.P., Pacharinsak, C., Long, C.T., Howard, A.M., Jampachaisri, K., Yeomans, D.C., Felt, S.A., (2011). Analgesic effects of tramadol, tramadol-gabapentin, and buprenorphine in an incisional model of pain in rats (Rattus norvegicus). Journal of the American Association for Laboratory Animal Science. 50, 192-197.
-
McLaughlin, C.R., Dewey, W.L., (1994). A comparison of the antinociceptive effects of opioid agonists in neonatal and adult rats in phasic and tonic nociceptive tests. Pharmacology Biochemistry and Behavior. 49, 1017-1023.
-
Mert, T., Gunes, Y., (2012). Antinociceptive activities of lidocaine and the nav1.8 blocker a803467 in diabetic rats. Journal of the American Association for Laboratory Animal Science. 51, 579-585.
-
Mert, T., Gunes, Y., Gunay, I., (2013). Comparison of actions of systemically and locally administrated local anaesthetics in diabetic rats with painful neuropathy. Fundamental & Clinical Pharmacology, 27, 161-168.
-
Pacharinsak, C., Smith, J.C., (2017). Handbook of Laboratory Animal Anesthesia and Pain Management: Rodents, CRC Press, Taylor & Francis Group.
-
Perkowski, S.Z.,Wetmore, L.A., (2006). The science and art of analgesia. In: Recent Advances in Veterinary Anesthesia and Analgesia: Companion Animals. Eds: Gleed, R.D., Ludders, J.W. Ithaca: International Veterinary Information Service (IVIS).
-
Pertovaara, A., Kauppila, T., Hämäläinen, M.M., (1996). Influence of skin temperature on heat pain threshold in humans. Experimental Brain Research. 107, 497-503. https://doi.org/10.1007/BF00230429
-
Porrello, E.R., Mahmoud, A.I., Simpson, E., Hill, J.A., Richardson, J.A., Olson, E.N., Sadek, H.A., (2011). Transient Regenerative Potential of the Neonatal Mouse Heart. Science. 331, 1078-1080.
-
Porrello, E.R., Mahmoud, A.I., Simpson, E., Johnson, B.A., Grinsfelder, D., Canseco, D., Mammen, P.P., Rothermel, B.A., Olson, E.N., Sadek, H.A., (2013). Regulation of neonatal and adult mammalian heart regeneration by the miR-15 family. Proceedings of the National Academy of Sciences. 110, 187-192.
-
Schlossmann, H.A., (1937). The relationship between age and the action of atropine and morphine. Journal of Pharmacology and Experimental Therapeutics. 60, 14-31.
-
Seymour, T.L., Adams, S.C., Felt, S.A., Jampachaisri, K., Yeomans, D.C., Pacharinsak, C., (2016). Postoperative analgesia due to sustained-release buprenorphine, sustained-release meloxicam, and carprofen gel in a model of incisional pain in rats (Rattus norvegicus). Journal of the American Association for Laboratory Animal Sciencei. 55, 300-305.
-
Swain, A., Nag, D.S., Sahu, S., Samaddar, D.P., (2017). Adjuvants to local anesthetics: Current understanding and future trends. World Journal of Clinical Cases. 5, 307-323.
-
Turner, P., Kirchain, S., Divincenti, L., Shomer, N., Nunamaker, E., Putta, S., Peterson, N., Pavek, T., Dennis, J., (2016). ACLAM position statement on pain and distress in research animals. Journal of the American Association for Laboratory Animal Science. 55, 821.
-
Turner, P.V., Pang, D.S., Lofgren, J.L., (2019). A review of pain assessment methods in laboratory rodents. Comparative Medicine. 69, 451-467.
-
Tzabazis, A., Klyukinov, M., Manering, N., Nemenov, M.I., Shafer, S.L., Yeomans, D.C., (2005). Differential activation of trigeminal C or Adelta nociceptors by infrared diode laser in rats: behavioral evidence. Brain Research. 1037, 148-156.
-
Van Sluyters, R.C., Obernier, A., (2004). Guidelines for the care and use of mammals in neuroscience and behavioral research. Contemporary Topics in Laboratory Animal Science. 43, 48-52.
-
Way, W.L., Costley, E.C., Leongway, E., (1965). Respiratory sensitivity of the newborn infant to meperidine and morphine. Clinical Pharmacology & Therapeutics. 6, 454-461.
-
Williams, W.O., Riskin, D.K., Mott, K.M., (2008). Ultrasonic sound as an indicator of acute pain in laboratory mice. Journal of the American Association for Laboratory Animal Science. 47, 8-10.
-
Zude, B.P., Jampachaisri, K., Pacharinsak, C., (2020). Use of flavored tablets of gabapentin and carprofen to attenuate postoperative hypersensitivity in an incisional pain model in rats (Rattus norvegicus). Journal of the American Association for Laboratory Animal Science. 59, 163-169.